

Why California Governor Gavin Newsom Keeps Making Homelessness Worse – OpEd
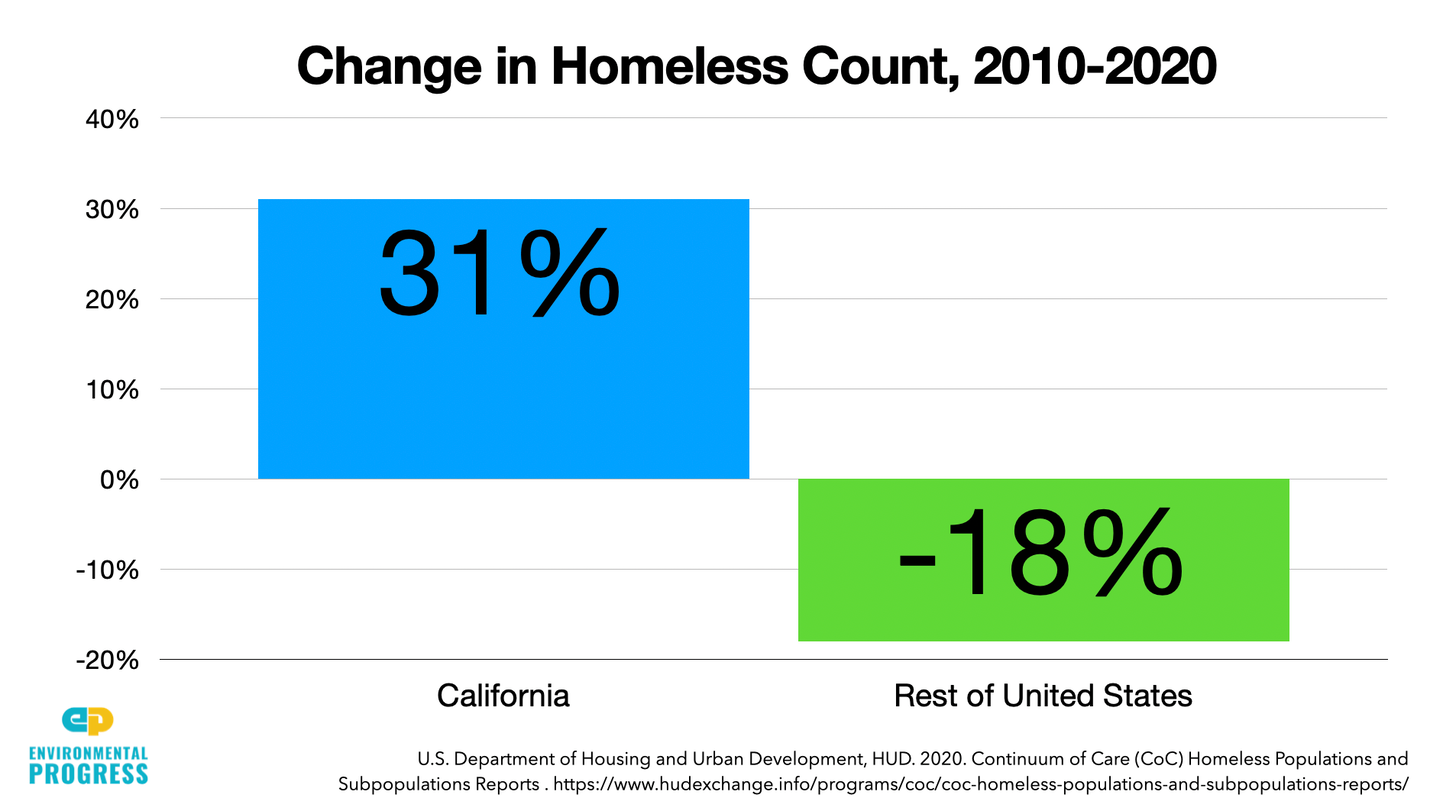
California saw its homeless population rise by 31 percent even as the number of homeless declined 18 percent in the rest of the United States between 2010 and 2020.
As a result, there are today 161,000 total homeless in California, with about 113,000 of them “unsheltered,” meaning they’re sleeping in tents on sidewalks, in parks, and alongside highways.
In response, California Governor Gavin Newsom proposed in a press conference today to spend another $12 billion on housing and services for homelessness.
Unfortunately, he is doubling down on the exact same solutions that have worsened the problem over the last decade.
While there are homeless people in other developed nations, there exists nothing like the open drug scenes and homeless encampments that have expanded across California in recent years.
Nor does there exist a drug overdose crisis approaching ours. In the early 2000s, around 17,000 people died from drug overdoses every year in the U.S.; by 2019, the rate of death had risen four-fold, to 70,000.
The way every other developed nation solves homelessness is through assertive case management, mandatory psychiatric care and drug treatment, and sufficient facilities of different kinds for different populations, from psychiatric hospitals to homeless shelters to permanent supportive housing.
California is overdue for a turn toward pragmatism and moderation when it comes to these issues. Californians do not want to return to mass incarceration nor to mental institutions like the kind depicted in “One Flew Over the Cuckoo’s Nest.” At the same time, we want and deserve public order, which is breaking down across the state.
There is a better way. To halt the degradation of human dignity and restore public order, California must provide, and require the homeless to use, basic shelter. And the limited housing for the homeless that exists should be available as a reward for positive behavioral outcomes, like overcoming addiction, taking one’s psychiatric medications, and working.
The Failure of Housing First
California’s homelessness crisis stems from the state’s lack of shelters, the lack of mandatory addiction and psychiatric services, and the absence of requirements to use them.
Two-thirds of the homeless in Los Angeles struggle with addiction or mental illness and half of San Francisco’s homeless struggle with both.
Newsom said he would put “billions” into mental health care, but California already spends 50 percent more per patient than the national average and has a 91 percent higher rate of mentally ill homeless than the rest of the U.S.
Newsom must know this. “There’s a shitload of money,” acknowledged the governor’s top mental health advisor, Dr. Thomas Insel, when we spoke by Zoom in late March
“We think $11 billion goes into California’s state mental health budget every year,” he said. “That makes California the number one in per capita spending in the United States. No state spends as much as we do. And yet when you look at the rankings by Mental Health America, and NAMI [National Alliance on Mental Illness], we’re not in the top half.”
The underlying problem is that Newsom and other California leaders insist on “Housing First,” and oppose expanding shelters and the requirement that people use them. According to Housing First, homeless people should just be given their own apartments with no requirement that they address their self-destructive behaviors.
As a result, there is a large and growing body of empirical evidence showing that Housing First may be increasing addiction and overdose deaths by making quitting drugs more difficult and using them easier.
“One potential risk [of Housing First’s harm reduction approach],” warned a multi-author review back in 2009, “would be worsening the addiction itself, as the federal collaborative initiative preliminary evaluation seemed to suggest.”
That’s what may have happened in 2020 with the program Newsom intends to scale up, Project Roomkey. During the pandemic, many homeless people were given their own hotel rooms where they overdosed and died. Had they been on the street, surrounded by people, they might have had their overdoses reversed.
One study found that, while the Housing First group kept people in housing longer, the comparison group saw greater reductions in alcohol consumption, problematic drug use, and greater improvements to mental health, after two years.
“One reason for the surprising results,” wrote the authors, “may be that aspects of the Housing First intervention, such as the privacy afforded by Housing First and harm reduction approach, might result in slower improvements around substance use and mental health.”
In 2018, the National Academies of Sciences, Engineering, and Medicine published a review of the scientific literature of Housing First. “On the basis of currently available research,” wrote the report’s authors, “the committee found no substantial evidence that [permanent supportive housing] contributes to improved health outcomes, notwithstanding the intuitive logic that it should.”
Housing First doesn’t even do a very good job of keeping people in housing. In the spring of 2021, a team of Harvard medical experts found that after ten years, just 12 percent of the homeless remained housed in Housing First housing.
Treatment First
California’s state auditor and the Legislative Analyst’s Office recognize the need for centralization, but say that California can improve its decentralized, county-by-county approach to homelessness through “coordination” by existing agencies.
Such coordination efforts have been tried repeatedly and failed for over three decades. Efforts for “coordination” create a collective action problem at the agency level. Employees respond to their superiors, not their peers. Everybody knows that when you want to get something done, you need a hierarchy, with a clear line of command and with leaders at the top who have both authority and accountability.
California’s homelessness crisis is also a problem of over-delegation. California counties have failed to solve the problem because they cannot solve it. Instead of governments providing such services directly, they give grants to nonprofit service providers who are unaccountable for their performance.
“There is no statutory requirement for government to address homelessness,” explained University of Pennsylvania researcher Dennis Culhane to me. “It’s mainly the domain of a bunch of charities who are unlicensed, unfunded, relatively speaking, run by unqualified people who do a shitty job.”
To solve the problem, the state of California needs to take over psychiatric and addiction services from the counties, significantly expand involuntary hospitalization for those who break the law, and break up the open air drug scenes and homeless encampments that endanger public safety.
The low-hanging fruit is getting the twenty-something year-old heroin and meth addicts off the street and into medically assisted treatment programs. The higher-hanging fruit is helping service-resistant people suffering from serious mental illness.
Researchers have found ways to use housing to reduce addiction. Between 1990 and 2006, researchers in Birmingham, Alabama, conducted clinical trials of abstinence-contingent housing for 644 homeless people with crack cocaine addictions. Two-thirds of participants remained abstinent after six months, a very high rate of abstinence, compared to other treatment programs.
In four randomized controlled trials, homeless people were given furnished apartments and allowed to keep them unless they failed a drug test, at which point they were sent to stay in a shelter. Sixty-five percent of participants completed the program. And participants in abstinent-contingent housing had better housing and employment outcomes than participants assigned housing for whom abstinence was not required.
In a major recent review of the literature, out of 176 controlled studies, 151 of them, or 86 percent, found contingency management to be effective for treating addiction, with the average effect size ranging from moderate to large. It significantly increased participation in therapy, a key component of addiction recovery.
Contingency management can also reduce psychiatric hospitalizations, improve financial management, and raise quality-of-life for the mentally ill suffering substance abuse disorder.
Participants who received the contingency management intervention were 2.4 times more likely to be abstinent than the control group, found a study using a large, randomized controlled trial among the seriously mentally ill, two-thirds of whom were homeless.
Contingency management is based on the well-supported psychological theory that concrete reinforcements, such as housing or gift cards, are necessary to encourage positive behaviors, such as abstinence, work, or accepting medical care.
Cal-Psych
A new state institution is required. Let’s call it Cal-Psych. It would be built as a skunkworks, wholly separate and superior to existing institutions, including health departments and health providers.
Cal-Psych’s CEO would be best-in-class and report directly to the governor. Cal-Psych would be built as a mobile and digital agency. Cal-Psych vans would have DMV embeds, tele-psychiatry, the ability to prescribe methadone or Suboxone, and instant access to psychiatric beds and drug treatment facilities. It would arrive immediately after people overdose from drugs to provide treatment.
Cal-Psych would have significant buying power and be able to move clients to where they need to be for treatment. It would be able to purchase psychiatric beds, board and care facilities, and treatment facilities from across the state. And it would be able to offer the mentally ill and those suffering from substance use disorders the treatment they need, and somewhere other than in an open air drug scene.
Cal-Psych would start in one city, learn rapidly, and then grow, ultimately taking over from the counties. We must learn from the mistakes of the past. We shut down state mental hospitals before we had created the alternative. Cal-Psych would be scaled up over time, gradually replacing various institutions that are currently doomed to failure.
Cal-Psych would do as much as legally, ethically, and practically possible to establish voluntary drug treatment and psychiatric care. It would also work with the courts and law enforcement to enforce involuntary care through assisted outpatient treatment and conservatorship.
Assisted outpatient treatment and conservatorship protect individual rights through the courts and allow non-jail and non-prison alternatives focused on psychiatric care. The ACLU has, in the past, done much good to protect rights, but they have taken an extreme position against conservatorship such that they may be actively contributing to the current crisis.
And while some counties may resist Cal-Psych, many will recognize that they cannot solve the problem. They may be happy to let go of the responsibility of caring for the chronically homeless, so long as they are reassured that they will not lose funding or control over county programs for those with milder mental illness such as depression, which are best handled at the county level.
Couldn’t Newsom use $12 billion to implement Cal-Psych?
When I spoke to Newsom’s advisor, Dr. Insel, he agreed that the state needed to make sweeping reforms. But, he said, “Everybody says the same thing to me. ‘You’re going to have to change the constitution because the way that we got to where we are was through a series of ballot measures.’”
But that’s not as daunting a challenge as it may seem. California governors raise money and pass ballot initiatives all the time, I pointed out. In fact, in the last 20 years, several major measures put on the ballot by former Governor Jerry Brown contributed to the state’s homeless addiction crisis.
Why hasn’t Newsom been pushing ballot initiatives? After Insel somewhat halfheartedly pointed to COVID-19 and the looming recall campaign, I scowled. He knew as well as I did that Newsom has been governor for more than a year before the pandemic and had been lieutenant governor and mayor for sixteen years before that.
Insel didn’t criticize Newsom directly, but when I read the transcript from our interview I was struck by how often he returned to one theme in particular.
“It’s been really hard to get any real leadership,” Insel said. “I don’t think money is the problem. I think it’s the leadership. . . . we need state leadership . . . There’s no state leadership. . . . We have to create state leadership. . . . I don’t think it’s a money problem. I think it’s a leadership problem.”
Ain’t that the truth.
First of all, let me state that my expressed opinions will be personal and not as a member of the Board of Directors for NAMI, Santa Clara County…This is an outstanding article! I am circulating it among my friends and colleagues. You correctly point out that much of housing and other amenities are simply given out by the State of California with no efforts at behavioral change required in return. Is it really an infringement on personal rights to require that a person take their meds as a condition for housing? I don’t think so. It’s better for the person and the State of California. I hope to see more from you regarding CA mental health issues in the future. If I can ever be of assistance feel free to contact me.