

COVID-19: Potential For Severe Secondary Waves In Asia – Analysis
Since the secondary virus waves started far earlier than expected and could be compounded by an adverse mutation, a new potential threat looms over Asia – as heralded by recent discoveries in Quezon City and Malaysia.
In the absence of deceleration, the accumulated confirmed cases worldwide could soar to 50-60 million and deaths to 1.5 to 1.7 million by the year-end. If Asian countries fail to “bend the curve” – that is, slow down the rapid acceleration of new COVID-19 cases – what we have seen in the past half a year could be a prelude to worse across the region.
In April, my first COVID-19 report focused on the outbreak in China and the belated mobilization and containment failure in the United States and Western Europe. My new report The Tragedy of More Missed Opportunities focuses on the estimated COVID-19 human costs and economic damage in the largest world economies, particularly in emerging and developing countries.
Since the anticipated ‘secondary waves’ began months earlier than expected, the coming months will test the public health systems of all nations. But some countries have better starting points.
Asia’s COVID-19 vulnerable countries – including the Philippines
Some countries will face the secondary waves from a position of resilience. They are countries that have managed to bend the curve,” with decelerating cumulative cases and lower positivity rates (the percentage of people who test positive for the virus of those overall who have been tested).
Other countries must struggle with the new waves from a position of vulnerability. They are countries that have failed to bend the curve, with accelerating cumulative cases and higher positivity rates.
In emerging and developing South, Southeast and East Asia, several countries are at risk. To gain a more realistic picture, let’s use population-adjusted data, linear scale and focus on those economies in which cases are still accelerating and positivity rate remains high (Figure 1).
Figure 1 Cumulative Confirmed COVID-19 Cases (Per 1 Million)
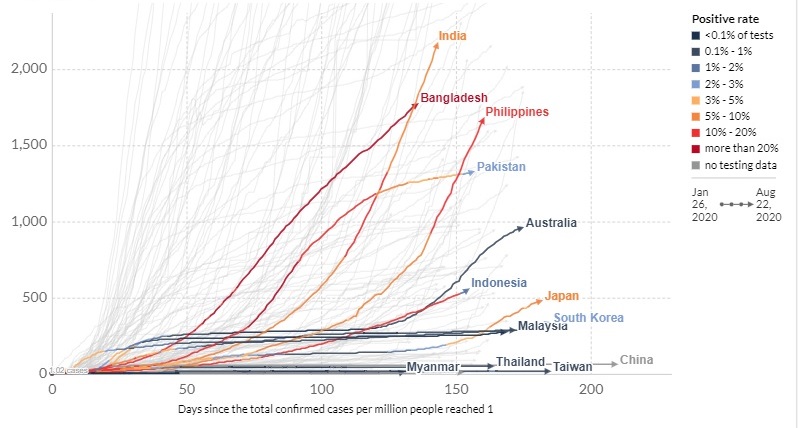
In this view, the primary risk group involves most of South Asia; that is, India, Bangladesh and Pakistan in which the number of cases continues to accelerate and positivity rate remains very high (around 5/10-20%).
The primary risk group also features Southeast Asia’s big growth engines, the Philippines and Indonesia, where numbers continue to accelerate alarmingly and positivity rates are as high as in South Asia.
However, these numbers significantly downplay effective realities in Pakistan where the current testing capacity is only half of that in India and the Philippines. The underassessments are likely to be even broader in Indonesia and Bangladesh, where the comparable capacity is barely a third relative to India and the Philippines.
In East Asia, case numbers continue to accelerate in Australia and Japan. Neither mobilized against the virus in time and effectively. However, unlike Australia, Japan’s testing capacity is very low for an advanced economy (only half relative to the Philippines) and thus likely disguises the true damage.
A new mutation, severe regional consequences
Recently, a “more infectious” COVID-19 strain was found in tested samples in Quezon City and in Malaysia. In the latter, the cases were discovered in clusters linked to cases imported from India and the Philippines.
This is a kind of development that was projected in my new report. It requires more research and aggressive vigilance. Here’s why: Not so long ago, a mutation was discovered in the protein that permits SARS-CoV-2 to enter cells possibly making it easier for the virus to spread.
Now, the original samples of the novel coronavirus out of Wuhan, China, were a variation that scientists call the “D” clade. Before March 1, over 90% of viral samples taken from patients were from D variation. Since March, however, a new “G” variation has been dominant (Figure).
Figure 2 Potential Transition of the Dominant Pandemic Form
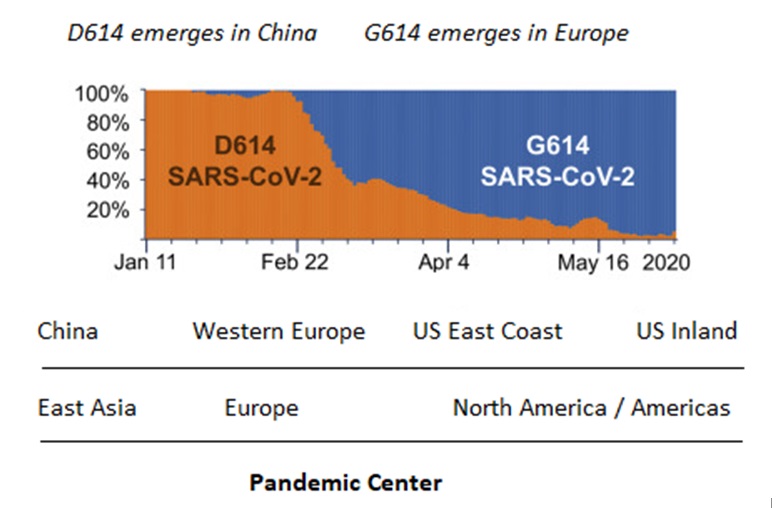
Though not conclusive yet, current evidence suggests there has been a global transition from the D to the G variation. Worse, the latter appears to increase COVID-19 infectivity.
Virulent implications?
If, as the researchers hypothesize, the G variation accelerated in Europe, it benefited from the global transportation hubs migrating across the Atlantic to New York City, which then seeded many of the outbreaks in the rest of the US, including locations where it is now running unchecked – as some investigative journalists also discovered by April.
There is a distressing implication associated with the presumed global transition from D to G variation. It could make the pandemic burden of emerging and developing economies more challenging than currently anticipated, particularly after normalization in the US and Europe, when quarantines, lockdowns and travel restrictions are phased out in the West.
Due to proximity and regional spillovers from the US, the G has been dominant in South America since March-April. Perhaps for similar reasons – proximity with Europe – it has also dominated infectivity in Africa.
In Asia and Oceania, the less-infective D was more dominant until recently. However, continued case acceleration and G variation dominance in several countries, coupled with the proliferation of secondary waves could change the status quo – for the worse.
Predecents matter
Historical precedents are instructive. Between 1918 and 1920, the Spanish flu is estimated to have infected 500 million people; every third person in the world at the time, while the death toll has been estimated at 17 to 50 million.
Yet, it was the second wave that proved far more deadly than the first. Facilitated by troop movements and logistical hubs during World War I, it spread over to North America, then Central and South America, and eventually to Africa Russia and Asia.
Today, the precedent of the Spanish flu should underscore the importance of proactive vigilance until effective vaccines, therapies or both are widely available.
If we still haven’t learned the “lesson of the second wave,” we will be forced to learn it over a major crisis – a more protracted pandemic and a multiyear global depression.
*Based on Dr Steinbock’s briefing of Aug 21 and his new report The Tragedy of More Missed Opportunities (https://www.differencegroup.net/covid19-report2)
Like what you read?
Please consider supporting Eurasia Review. Thank you for your consideration!