

Patenting The Cure: At What Cost? – Analysis
By Aarshi Tirkey
The world at large is banking on a cure to treat and eradicate the COVID-19 disease. Research efforts and clinical trials are ongoing in various countries to test, develop and launch new medicines, vaccines and therapeutics. In this context, there has been growing debate around whether access to a cure — once found — could be impeded or restricted through the monopoly rights granted by patents.
Patents are a form of intellectual property right (IPR) that provides inventors a 20-year monopoly over their creations. During this period, patent holders have the exclusive right to manufacture and sell their invention, or license it to a third party in return for royalties or license fees. The raison d’être for patent protection is to enable an inventor to recuperate R&D costs, and to incentivise future innovation and research. This becomes important since the cost of bringing new medicines and vaccines cost pharmaceutical companies $1 billion or more.
However, the existing regime for patent protection has in turn encouraged profiteering and distorted the development and pricing of new drugs. Often, costs for treatments are exorbitantly high and research in pharmaceutical companies are oriented towards diseases that affect the affluent. Further, rather than incentivising innovation, pharmaceuticals have used patents to privatise and lock up knowledge commons by filing for frivolous secondary patents and by lobbying against generic medicines.
As such, government policies on patent regulations attempt to balance incentive for research on one hand, with societal benefits and equitable access on the other. A suitable national policy response to this question becomes all the more important in the context of the pandemic. If a vaccine or a treatment is to be created, is there a possibility that patent rights could restrict access to the cure across the world? Much depends on a government’s willingness to tweak patent rules, and its openness to adopt new mechanisms that encourage research and collaboration, and dismantle existing barriers to access.
Figure 1: COVID-19 vaccines in development around the world
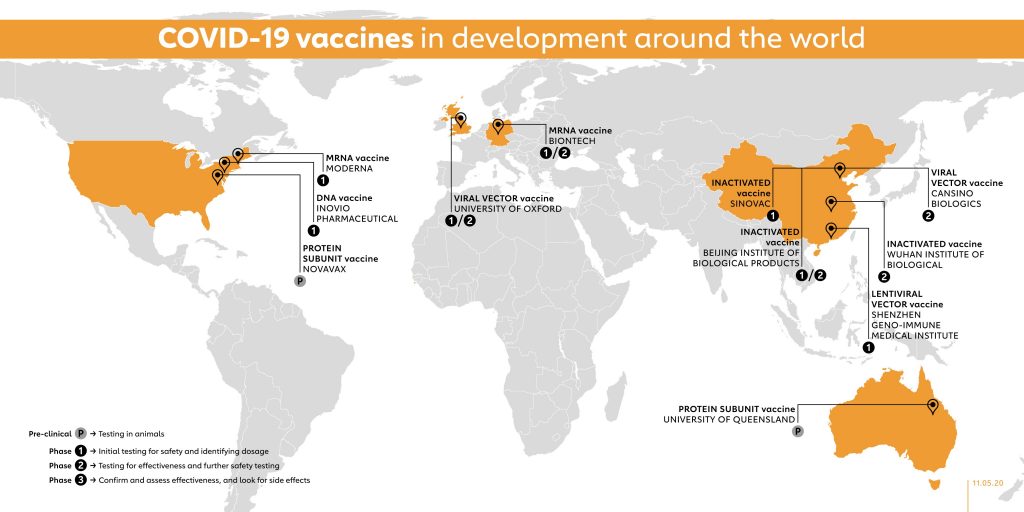
The onus of formulating a suitable response to accommodate these considerations falls on developed countries, since they are leading the race on vaccine and antiviral drug development. With specific reference to vaccines, figure 1 provides an overview of institutions and companies that are developing them across the world. Figure 2, breaks down vaccine developers by country and categorises them as public (non-profit), private and academic. More than 70% vaccine research efforts are being led by industrial or private firms. Majority of these developers are based in North America. Given the resources, expertise and advanced equipment available with developed countries, it is highly likely that a treatment to COVID-19 will be found from here.
However, countries like the US and major private pharmaceutical companies have been resistant to join efforts to collaborate and ensure equitable access to drugs and vaccines. For instance, one suggestion to facilitate the creation of medicines and vaccines is to launch a global patent pool. This is a mechanism that allows owners and innovators to aggregate complementary patents and license them, thereby reducing access time and cost for developing countries. A 2005 study on the SARS outbreak recognised that this mechanism could be an essential tool to help create vaccines. This method exists in practice under the United Nations-backed Medicines Patent Pool (MPP) which works to increase access to life-saving medicines for low- and middle-income countries.
As a result, in May 2020, a European Union lead resolution at the World Health Organisation (WHO) — co-sponsored by countries like India and the UK — committed to global solidarity and international cooperation to ensure access to medicines, vaccines and medical equipment. Some of the methods enumerated in the resolution included voluntary pooling of patents and the use of existing trade rules to scale up manufacturing and distribution of treatment and vaccines — once they are created. However the US, in its statement, opposed these provisions and “disassociated” itself from it. It reasoned that they do not capture negotiated trade rules, and could affect Washington’s ability to incentivise new drug development. Major pharmaceutical companies such as Pfizer and GlaxoSmithKline (GSK) have also expressed resistance towards joining such initiatives, with the former terming them as “dangerous.”
This is a troublesome development, since the US has the highest number of vaccine trials as of today. One needs to look no further than the sordid history of the HIV/AIDS epidemic and how the exorbitant pricing of its treatment caused immense hardship to many. At the height of the HIV/AIDS epidemic, the three-stage antiretroviral therapy cost a whopping $10,000. Back then, this pricing was denounced as a “shocking and monstrous iniquity,” and the problem of high prices and inaccessibility of drugs was blamed on Western companies, who controlled patents. A more recent example can be found closer home in India, where 127,000 infants die from pneumonia every year. Though Pfizer’s pneumonia vaccine is provided at a subsidised cost, it continues to be unaffordable for many.
The traditional rules for allocating resources and ownership under international law rely on the concept of sovereignty. Countries have sovereignty over resources and samples found in their territory; and this similarly extends to medicines and vaccines manufactured in their territory. As such, the 2009 H1N1 epidemic demonstrated how developed countries that have control over production and supply over vaccines, would respond (or rather, not respond) to humanitarian concerns of developing countries. During the H1N1 epidemic, Canada refrained from committing to a pledge to donate the vaccines. The US and Australia mandated their manufacturers to fulfill domestic requirements first, before servicing donation obligations. This gravely affected the timing and amount of vaccines available for developing countries. The scramble to stock supplies and prioritise domestic requirements, placed developing countries in a long line to wait for the cure to reach them.
The current regime on vaccine and medicine distribution relies on ad hoc, reactive and non-binding arrangements that preserve national freedom of action. Ad hoc mechanisms here refer to bilateral donation programmes, provision of vaccines by international organisations (WHO and UNICEF), and public private mechanisms, such as GAVI alliance and the Clinton Global Initiative. This is not to criticise the utility and objectives of such programmes. However, a country’s participation in such voluntary mechanisms fosters the notion that it has done enough to address humanitarian concerns and meet its obligations as a responsible global actor. This, in turn, defers any real discussion on legal or binding arrangements to ensure equitable access to vaccines.
The response of countries to COVID-19 is in stark contrast with the response of the global scientific community. It is a given that the free flow of information, research and data will vastly expedite the development of a cure. In an effort to accelerate such efforts, the global scientific community has been particularly forthcoming in sharing their knowledge and research findings. Several leading medical journals have categorised all relevant publications on COVID-19 as open access material. Scientists and institutions have also come forward to undertake the Open Covid Pledge to promise the free use of their intellectual property. As this Lancet article notes, “scientific borders have been flung open and barriers torn down”… and “spawned a new era of scientific collaboration, open discourse, and efficiency.”
On the other hand, the response of countries leaves much to be desired. An open letter, from world leaders and public figures urges that any vaccine against Covid-19 should be patent-free, produced at scale and made available at no cost to people everywhere. COVID-19 has already been dubbed as the “the great unequaliser,” as it exacerbates disparities in income, wealth and opportunities. These disparities could extend to the global level if equitable access to vaccines and treatment is not guaranteed. The need for global cooperation and collaboration to diversify production and manufacturing to address emergency health situations has been recognised long before. Negotiations are needed to foster consensus on collective action, so as to ensure that the cure is available to all and that the treatment — like the disease — does not disproportionately harm the most vulnerable communities in the world.
Like what you read?
Please consider supporting Eurasia Review. Thank you for your consideration!